October 2015 |
drinkanddrugsnews
| 7
Read the full version online at:
lots of natural weed supplies in the world) would suggest that the
market for SC products should be dying. And yet they represent the
fastest growing group of novel psychoactive drugs reported to
international monitoring agencies like the EMCDDA. One reason is
that when one set of synthetic cannabinoids is regulated, there’s a
whole truck full waiting to be dissolved in acetone and sprayed on
damiana and lettuce leaf, dried, packaged and sold for huge profits
with no need for elegant hydro set-ups, electricity and water.
B
ut why is there still demand? Why use a less desirable
product when a preferable one is usually available? At least
in some cases, it will be to avoid workplace drug screens.
Working in a prison, I know these products have had real
currency, and the same could be said for those in transport, mining
and other risk-critical areas. But it’s not just avoidance of detection
that can be an issue – it’s also price, potency and bang for buck,
because over the last decade, high potency weed has increased in
price relative to other drugs in many parts of the world. At a mean
price of around €10/gram (and most people getting three to four
joints out of gram), pot smoking has become an expensive habit.
For some people, using a more potent but less desirable product
might just be down to economics. I bumped into a guy in a head
shop in London, who was buying 3gm of cherry bomb for £25. I
asked ‘wouldn’t you rather smoke some nice weed?’ ‘Yeah,’ he said,
‘I’m a weed man, but I only get three spliffs from a gram. I can
get 25 spliffs out of this. I use it to sleep – saves on my use of
nice weed.’
Two minutes later in walked a mother in her mid-30s with her
nine-year-old son: ‘I’ll have the usual – three blueberry bags please.’
So it is out there and people are using it. And sometimes users end
up in the ER room, agitated, sweaty, paranoid and psychotic.
I also worry that, given all we know about the harms of early
onset cannabis use impacting on the developing brain and
increasing the risk of schizophrenia, use of SCs by young people
might be a real public health issue. I have to remind them, ‘before
you try and expand your brain, you have to let it grow.’
This year GDS is continuing its assessment of synthetic cannabis
products. We’ll be looking at the risks of getting dependent,
whether or not people get withdrawal, and whether vaporisers and
potent new preparations are leading to a whole new range of
health risks – or benefits.
Dr AdamWinstock is the founder of Global Drug Survey and a
consultant psychiatrist, addiction medicine specialist and
researcher, based in London.
To contribute experiences to GDS2015, visit
More information at the GDS YouTube channel:
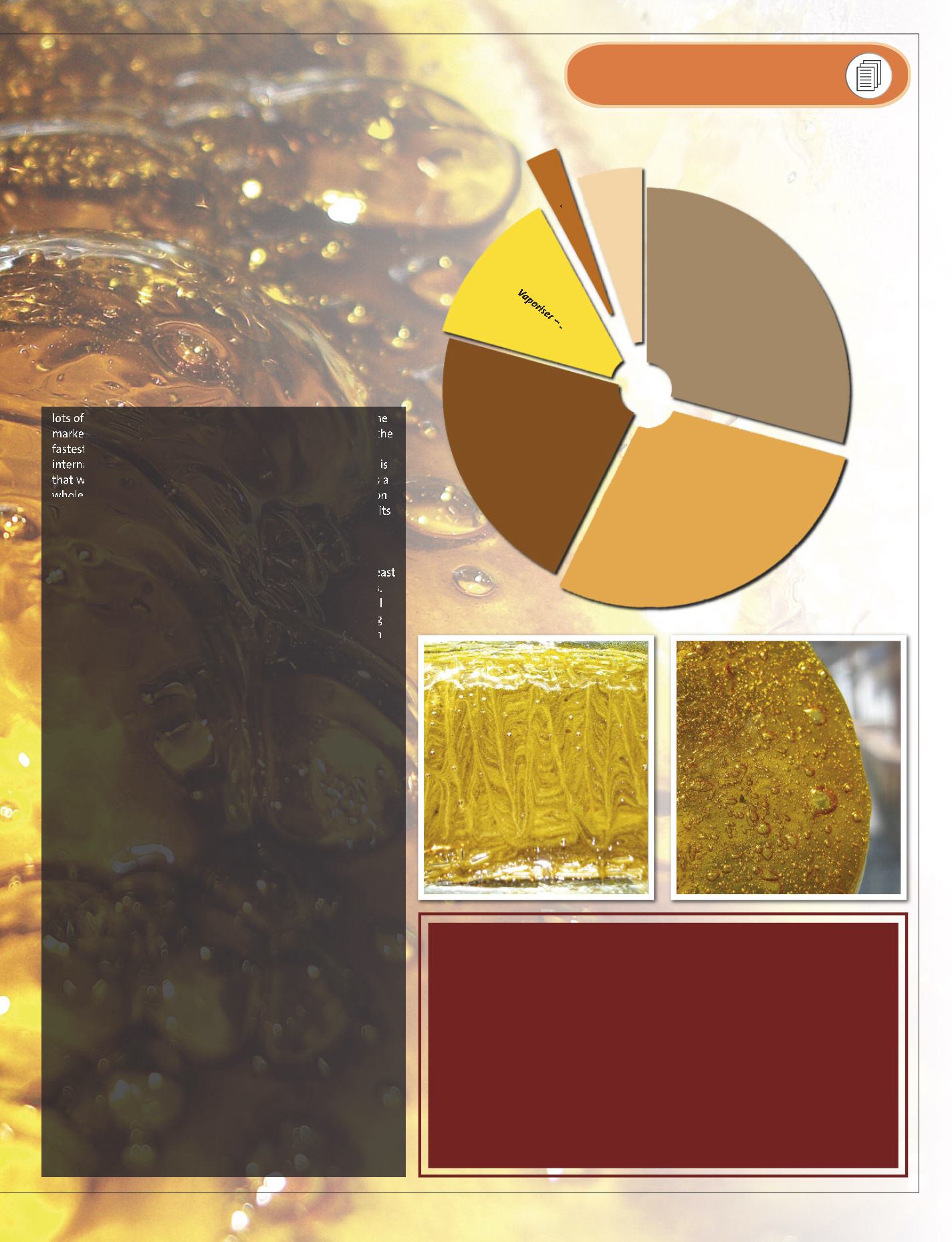
Oral use – 3%
Bong/water pipes – 5%
Vaporiser – 13%
Hot knife/nail – 22%
Vape pen – 28%
Joints with tobacco – 29%
BHO: QUESTIONS WE NEED TO ASK
Will the use of more potent forms of cannabis such as BHO lead to higher rates
of dependence, unwanted psychological experiences and withdrawal?
Could the adoption of BHO in countries dominated by tobacco-associated
routes of administration allow safer routes of use?
Could BHO broaden consumer choice and allow both medicinal and
recreational cannabis users to obtain their preferred THC/CBD preparations?
Could the promotion of vaping technology attract cannabis-naïve users to try
the drug?
Will BHO be more or less commercially attractive to dealers/manufacturers?
Should the risks of BHO production (explosions) support the public health
dissemination of safer production methods avoiding the use of volatile solvents?
COMMON METHODS
OF BHO CONSUMPTION


